1st MTP Arthritis / Dorsal Bunion / Hallux Rigidus / Big Toe Arthritis
Hallux Rigidus (HR) refers to stiffness (rigidus) of the joint at the base of the great toe (hallux).
Hallux Rigidus, also known as big toe arthritis, is quite common.
The exact cause is unknown and does not usually follow injury. It is one of the most common joints in the body to wear out as people get older. It is probably of little surprise that this joint is prone to arthritis as forces up to twice the body weight passes through the great toe MTPJ during walking.

Symptoms of Hallux Rigidus
Hallux Rigidus causes pain and stiffness. This may limit walking distance, and compromise work and recreational activities. Bony spurs (osteophytes) develop around the great toe MTPJ and can cause pain by rubbing against tight fitting shoes. In an attempt to off–load the painful great toe, some people will preferentially walk on the outer border of the foot, causing transfer pain to the lesser toes.
Initially, pain can be managed by orthotics and shoe modifications. Anti inflammatory medication can help for certain situations and occasionally injections are useful.
But like many things in our body the wearing out process catches up and symptoms become hard to manage.
Fortunately we have two minimally invasive options to help relieve pain and increase function.
Non Operative Treatment
The main aims are to relieve pain and decrease loading and movement through the great toe MTPJ. In its mildest form, Hallux Rigidus may not need operative treatment.
Simple lifestyle and activity modifications, weight loss, the use of a walking aid, taking pain killers (panadol and anti–inflammatories) and wearing appropriate shoe wear and orthotics (stiff insoles or shoes with a rocker bottom) can all be helpful. High heels and shoes with a narrow toe box should be avoided.
Finally, a cortisone injection may offer relief of inflammation but as with most treatments, the degree and extent of relief varies from patient to patient.
Operative Treatment
Surgery is considered when the above measures fail.
There are 2 main surgical options to relieve pain and improve quality of life. These include Cheilectomy and arthrodesis or fusion of the MTPJ.
The best option for an individual patient depends on many factors including the severity of arthritis, the age and functional demands of the patient and the presence of arthritis in adjacent joints. The final choice is a joint decision between surgeon and patient.
1. Cheilectomy
If the HR is mild, affecting only the upper part of the joint, this upper portion may be trimmed and the joint washed out. This is often combined with a realignment procedure (Moberg osteotomy) of the bone at the base of the great toe. This combination can provide long lasting pain relief with improved movement of the great toe in the appropriate patient. In 10–20% of patients, the arthritis is progressive and symptoms may return to a point where further procedures may be required.
Until late in the disease process most of the pain come from bone spurs which grow on top of the joint. These cause impingement while walking, generating sharp pains. For ladies, this makes wearing heels very painful. So removing these spurs and making a minor adjustment to the next bone along will relieve the impingement, increase movement and relieve the pain.
This surgery is performed as a day case and walking is allowed as soon as comfortable. Most patients are back in shoes after a week or two.
Like most things in the foot the biological healing will take about 3 months so the final result will not be seen until then. However after about 4 weeks most patients are already feeling better than before.
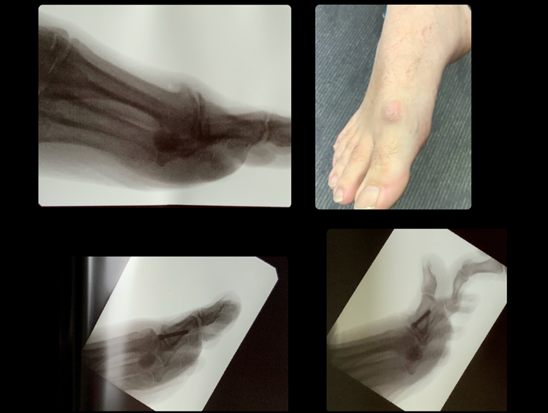
You will see from the images below the patient has a large lump on the top of the foot on the photo and X-ray. The below images show the post operative images with the bone removed. You can also see the movement of the joint afterwards on the bottom right image. You can see below this the wound healing and minimally invasive incisions.

2. MTPJ arthrodesis (fusion)
When the joint has totally worn out a cheilectomy will no longer help. Usually by this time the joint has almost totally stiffened.
A fusion of the joint is the preferred treatment at this stage. Because the joint is stiff anyway no extra movement is lost. So the patient is the same as before surgery, just without the pain.
There is another joint towards the tip of the toe which can take over the main joint function. This is also done via a minimally invasive approach with the wound being similar to the cheilectomy.


Risks and Complications
As a guide 90–95% of patients will derive significant benefit and will be happy with the surgical result. Less than 5–10% will develop a complication that may require further intervention.
These include: wound healing problems, infection, damage to nerves and blood vessels, incomplete relief of symptoms, and in the case of arthrodesis, failure of the bones to knit together, requiring further surgery.
Operation Information & Post–Op Guidelines
Surgery for Hallux Rigidus using minimally invasive techniques
HOSPITAL STAY
| In Hospital | 1 Day/Night |
DRESSINGS
| Bandages | 14 Days |
MOBILISATION
| Elevate foot | 7 Days |
| Crutches | 7 Days |
| Partial weight bearing | 1 Week |
WORK/DRIVING
| NO driving | 2 Weeks |
Off Work
|
1–2 Weeks |
RECOVERY
| Walking freely | ~4–6 Weeks |
| Post operative shoe | 4 Weeks |
| Foot remains swollen | 12 Weeks |
| Final result | 16 Weeks |
Take regular analgesia 4–6 hourly throughout Post–Operative period (14 days).
Take 2 Panadol 1 hour before Post Op visit.
These timeframes should be used as a guide only and may vary for individual patients based on the nature or extent of the actual surgery performed and individual circumstances. Please contact Mr Blackney′s rooms on (03) 9417 0762 if you require further information.